

PART 15: Disorders of the Joints and Adjacent Tissues
SECTION 2 Disorders of Immune-Mediated Injury
e40 Atlas of the Vasculitic Syndromes
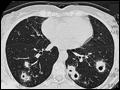
 | Figure e40-1 Bilateral nodular infiltrates seen on computed tomography of the chest in a 40-year-old woman with granulomatosis with polyangiitis (Wegener's). |
view large |
 | Figure e40-2 Computed tomography of the chest in two patients with granulomatosis with polyangiitis (Wegener's) demonstrating (A) single and (B) multiple cavitary lung lesions. |
view large |
 | Figure e40-3 Bilateral ground-glass infiltrates due to alveolar hemorrhage from pulmonary capillaritis as seen in the same patient by (A) chest radiograph and (B) computed tomography. This manifestation can occur in granulomatosis with polyangiitis (Wegener's) or microscopic polyangiitis. |
view large |
 | Figure e40-4 Computed tomography of the chest demonstrating a dense infiltrate with air bronchograms involving a segment of the right upper lobe due to bacterial pneumonia in an immunosuppressed patient with granulomatosis with polyangiitis (Wegener's). Collapse of the left upper lobe secondary to endobronchial stenosis from granulomatosis... |
view large |
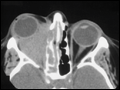 | Figure e40-5 Computed tomography of the orbits in a patient with granulomatosis with polyangiitis (Wegener's), who presented with right-eye proptosis. The image demonstrates inflammatory tissue extending from the ethmoid sinus through the lamina papyracea and filling the orbital space. |
view large |
 | Figure e40-6 Computed tomography of the sinuses in two patients with granulomatosis with polyangiitis (Wegener's) (A) Mucosal thickening of the bilateral maxillary sinuses and a perforation of the nasal septum. (B) Osteitis with obliteration of the left maxillary sinus in a patient with long-standing sinus... |
view large |
 | Figure e40-7 Computed tomography of the chest demonstrating a large pericardial effusion in a patient with Churg-Strauss syndrome. Cardiac involvement is an important cause of morbidity and mortality in Churg-Strauss syndrome and can include myocarditis, endocarditis, and pericarditis. |
view large |
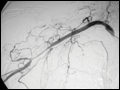
 | Figure e40-8 Arteriogram of a 40-year-old man with polyarteritis nodosa demonstrating microaneurysms in the hepatic circulation. |
view large |
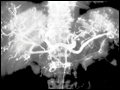
 | Figure e40-9 Cerebral arteriogram demonstrating beading along branches of the internal carotid artery in a patient with isolated central nervous system vasculitis. |
view large |
 | Figure e40-10 Upper-extremity arteriogram demonstrating a long stenotic lesion of the axillary artery in a 75-year-old female with giant cell arteritis. |
view large |
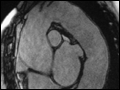 | Figure e40-11 Magnetic resonance imaging demonstrating extensive aneurysmal disease of the thoracic aorta in an 80-year-old female. The patient had been diagnosed with biopsy-proven giant cell arteritis 10 years prior to presenting with this aneurysm. |
view large |
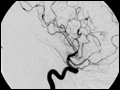
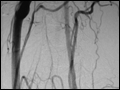 | Figure e40-12 Arteriogram of the aortic arch demonstrating complete occlusion of the left common carotid artery just after its origin from the aorta. This 20-year-old female presented with syncope and was subsequently diagnosed with Takayasu's arteritis. |
view large |
 | Figure e40-13 Arteriogram demonstrating stenosis of the abdominal aorta in a 25-year-old female with Takayasu's arteritis. |
view large |
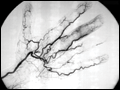 | Figure e40-14 Arteriogram of the hand demonstrating arterial skip lesions and vessel cutoffs in a patient with cryoglobulinemia due to multiple myeloma. |
view large |
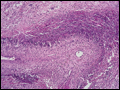 | Figure e40-15 Lung histology in granulomatosis with polyangiitis (Wegener's). This lung biopsy shows areas of geographic necrosis with a border of histiocytes and giant cells. There is also vasculitis with neutrophils, lymphocytes, and giant cells infiltrating the wall of an artery. |
view large |
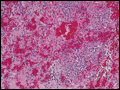 | Figure e40-16 Lung histology in microscopic polyangiitis. This lung biopsy demonstrates hemorrhage in the alveolar spaces due to capillaritis in a patient with microscopic polyangiitis. Similar findings can also be seen in granulomatosis with polyangiitis (Wegener's) and less commonly in Churg-Strauss syndrome. |
view large |
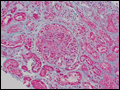 | Figure e40-17 Kidney biopsy in granulomatosis with polyangiitis (Wegener's). This renal biopsy shows a crescentic and necrotizing glomerulonephritis. These findings were focal and segmental with normal and scarred glomeruli also being found in the biopsy. By immunofluorescence and electron microscopy, no immune deposits were present,... |
view large |
 | Figure e40-18 Sural nerve biopsy in polyarteritis nodosa. This sural nerve biopsy was performed in a patient with polyarteritis nodosa, who had presented with a mononeuritis multiplex. Neutrophils are seen infiltrating all layers of this medium-sized vessel, which resulted in vessel occlusion and nerve infraction. |
view large |
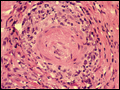
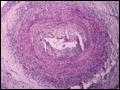 | Figure e40-19 Temporal artery biopsy in giant cell arteritis. This temporal artery biopsy demonstrates a panmural infiltration of mononuclear cells and lymphocytes that are particularly seen in the media and adventitia. Scattered giant cells are also present. |
view large |
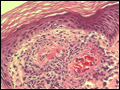 | Figure e40-20 Cutaneous vasculitis. This skin biopsy reveals two arterioles beneath the dermis with a neutrophilic inflammatory infiltrate in and around the vessel wall with leukocytoclasis (nuclear debris). While such features are diagnostic of vasculitis, they can be seen in a variety of settings and are not specific for any single disease. |
view large |
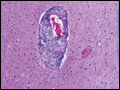 | Figure e40-21 Granulomatous primary angiitis of the central nervous system. This brain biopsy demonstrates a medium-sized artery with granulomatous inflammation present within the vessel wall indicative of a granulomatous vasculitis. This patient presented with progressive headache, clinical and radiographic features of a stroke, and had... |
view large |