

PART 11: Disorders of the Respiratory System
SECTION 1 Diagnosis of Respiratory Disorders
e34 Atlas of Chest Imaging
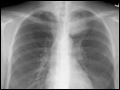
 | Figure e34-1 Normal chest radiograph—review of anatomy.1. Trachea. 2. Carina. 3. Right atrium. 4. Right hemidiaphragm. 5. Aortic knob. 6. Left hilum. 7. Left ventricle. 8. Left hemidiaphragm (with stomach bubble). 9. Retrosternal clear space. 10. Right ventricle. 11. Left hemidiaphragm (with stomach bubble). 12. Left upper lobe bronchus. |
view large |
 | Figure e34-2 Normal chest tomogram—note anatomy. 1. Superior vena cava. 2. Trachea. 3. Aortic arch. 4. Ascending aorta. 5. Right mainstem bronchus. 6. Descending aorta. 7. Left mainstem bronchus. 8. Main pulmonary artery. 9. Heart. 10. Esophagus. 11. Pericardium. 12. Descending aorta. |
view large |
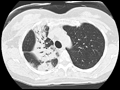
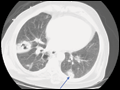
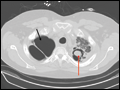
 | Figure e34-3 CT scan demonstrating left upper lobe collapse. The patient was found to have an endobronchial lesion (not visible on theCT scan) resulting in this finding. The superior vena cava (black arrow) is partially opacified by intravenous contrast. |
view large |
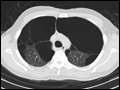
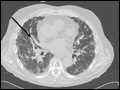
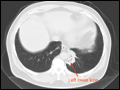 | Figure e34-4 CT scan revealing chronic left lower lobe collapse. Note dramatic volume loss with minimal aeration. There is subtle mediastinal shift to the left. |
view large |
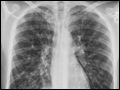
 | Figure e34-5 Left upper lobe scarring with hilar retraction with less prominent scarring in right upper lobe as well. Findings consistent with previous tuberculosis infection in an immigrant from Ecuador. |
view large |
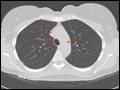
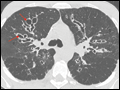
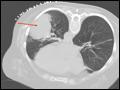
 | Figure e34-6 Apical scarring, traction bronchiectasis (red arrow), and decreased lung volume consistent with previous tuberculosis infection. Findings most significant in left lung. |
view large |
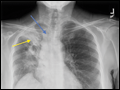
 | Figure e34-7 Chest x-ray (CXR) demonstrating right upper lobe collapse (yellow arrow). Note the volume loss as demonstrated by the elevated right hemidiaphragm as well as mediastinal shift to the right. Also apparent on the film are an endotracheal tube (red arrow) and a central venous catheter (black... |
view large |
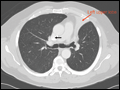
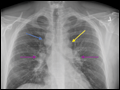
 | Figure e34-8 Opacity in the right upper lobe. Note the volume loss as indicated by the elevation of the right hemidiaphragm, elevation of minor fissure (yellow arrow) and deviation of the trachea to the right (blue arrow). |
view large |
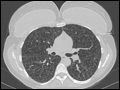
 | Figure e34-9 CT scan of the same right upper lobe opacity. Note the air bronchograms and areas of consolidation. |
view large |
 | Figure e34-10 Emphysema with increased lucency, flattened diaphragms (black arrows), increased AP diameter, and increased retrosternal clear space (red arrow). |
view large |
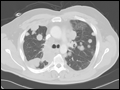
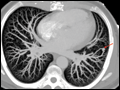
 | Figure e34-11 CT scan of diffuse, bilateral emphysema. |
view large |
 | Figure e34-12 CT scan of bullous emphysema. |
view large |
 | Figure e34-13 —note multiple thin-walled parenchymal cysts. |
view large |
 | Figure e34-14 Two cavities on posteroanterior (PA) and lateral CXR. Cavities and air-fluid levels identified by blue arrows. The smaller cavity is in the right lower lobe (located below the major fissure, identified with the yellow arrow) and the larger cavity is located in the right... |
view large |
 | Figure e34-15 CT scan of parenchymal cavity. |
view large |
 | Figure e34-16 Thick-walled cavitary lung lesions. The mass in the right lung has thick walls and advanced cavitation, while the smaller nodule on the left has early cavitary changes (arrow). This patient was diagnosed with Nocardia infection. |
view large |
 | Figure e34-17 Mild congestive heart failure. Note the Kerley B lines (black arrow) and perivascular cuffing (yellow arrow) as well as the pulmonary vascular congestion (red arrow). |
view large |
 | Figure e34-18 Pulmonary edema. Note indistinct vasculature, perihilar opacities, and peripheral interstitial reticular opacities. While this is an anteroposterior film making cardiac size more difficult to assess, the cardiac silhouette still appears enlarged. |
view large |
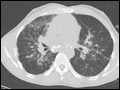
 | Figure e34-19 CXR demonstrates reticular nodular opacities bilaterally with small lung volumes consistent with usual interstitial pneumonitis (UIP) on pathology. Clinically, UIP is used interchangeably with idiopathic pulmonary fibrosis (IPF). |
view large |
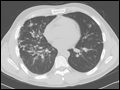
 | Figure e34-20 CT scan of usual interstitial pneumonitis (UIP), also known as idiopathic pulmonary fibrosis (IPF). Classic findings include traction bronchiectasis (black arrow) and honeycombing (red arrows). Note subpleural, basilar predominance of the honeycombing. |
view large |
 | Figure e34-21 (A) PA chest film—note presence of paratracheal (blue arrow), aortopulmonary window (yellow arrow) and hilar (purple arrows) lymphadenopathy. (B) Lateral film—note hilar lymphadenopathy (purple... |
view large |
 | Figure e34-22 Sarcoid—CT scan of stage I demonstrating bulky hilar and mediastinal lymphadenopathy (red arrows). |
view large |
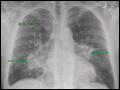 | Figure e34-23 Sarcoid—CXR of stage II. (A) PA film with hilar lymphadenopathy (green arrows) and parenchymal changes. (B) Lateral film with hilar adenopathy (green arrow) and parenchymal changes |
view large |
 | Figure e34-24 Sarcoid—CT scan of stage II (calcified lymphadenopathy, parenchymal infiltrates). |
view large |
 | Figure e34-25 Sarcoid—CT scan of stage II (nodular opacities tracking along bronchovascular bundles). |
view large |
 | Figure e34-26 Sarcoid—stage IV with fibrotic lung disease and cavitary areas (yellow arrow). |
view large |
 | Figure e34-27 Right middle lobe opacity illustrates major (black arrow) and minor fissures (red arrows) as well as the "silhouette sign" on the right heart border. |
view large |
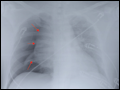
 | Figure e34-28 Right lower lobe pneumonia—subtle opacity on PA film (red arrow), while the lateral film illustrates the "spine sign" (black arrow) where the lower spine does not become more lucent. |
view large |
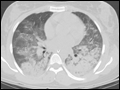
 | Figure e34-29 CT scan of diffuse, bilateral "ground-glass" opacities. This finding is consistent with fluid density in the alveolar space. |
view large |
 | Figure e34-30 CXR reveals diffuse, bilateral alveolar opacities without pleural effusions, consistent with acute respiratory distress syndrome (ARDS). Note that the patient has an endotracheal tube (red arrow) and a central venous catheter (black arrow). |
view large |
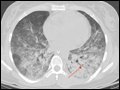
 | Figure e34-31 CT scan of ARDS demonstrates "ground-glass" opacities with more consolidated areas in the dependent lung zones. |
view large |
 | Figure e34-32 Three examples of air bronchograms (red arrows) on chest CT. |
view large |
 | Figure e34-33 Cystic fibrosis with bronchiectasis, apical disease. |
view large |
 | Figure e34-34 CT scan of diffuse, cystic bronchiectasis (red arrows) in a patient with cystic fibrosis. |
view large |
 | Figure e34-35 CT scan of focal right middle lobe and lingular bronchiectasis (yellow arrows). Note that there is near total collapse of the right middle lobe (red arrow). |
view large |
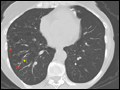 | Figure e34-36 "Tree in bud" opacities (red arrows) and bronchiectasis (yellow arrow) consistent with atypical mycobacterial infection. "Tree in bud" refers to small nodules clustered around the centrilobular arteries as well as increased prominence of the centrilobular branching. These findings are consistent with... |
view large |
 | Figure e34-37 Large right pneumothorax with near complete collapse of right lung. Pleural reflection highlighted with red arrows. |
view large |
 | Figure e34-38 Basilar pneumothorax with visible pleural reflection (red arrows). Also note, patient has subcutaneous emphysema (yellow arrow). |
view large |
 | Figure e34-39 CT scan of large right-sided pneumothorax. Note significant collapse of right lung with adhesion to anterior chest wall. Pleural reflection highlighted with red arrows. The patient has severe underlying emphysema. |
view large |
 | Figure e34-40 Small right pleural effusion (red arrows highlight blunted right costophrenic angles) with associated pleural thickening. Note fluid in the major fissure (black arrow) visible on the lateral film as well as the meniscus of the right pleural effusion. |
view large |
 | Figure e34-41 Left pleural effusion with clear meniscus seen on both PA and lateral chest radiographs. |
view large |
 | Figure e34-42 Asbestosis. Note calcified pleural plaques (red arrows), pleural thickening (black arrow), and subpleural atelectasis (green arrows). |
view large |
 | Figure e34-43 Left upper lobe mass, which biopsy revealed to be squamous cell carcinoma. |
view large |
 | Figure e34-44 Solitary pulmonary nodule on the right (red arrow) with a spiculated pattern concerning for lung cancer. Note also that the patient is status-post left upper lobectomy with resultant volume loss and associated effusion (black arrow). |
view large |
 | Figure e34-45 Metastatic sarcoma. Note the multiple, well-circumscribed nodules of different size. |
view large |
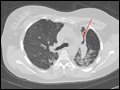
 | Figure e34-46 Left lower lobe lung mass (red arrow) abutting pleura. Biopsy demonstrated small cell lung cancer. |
view large |
 | Figure e34-47 CT scan of soft tissue mass encircling the trachea (red arrow) and invading tracheal lumen. Biopsy demonstrated adenoid cystic carcinoma (cylindroma). |
view large |
 | Figure e34-48 Mycetoma. Fungal ball (red arrow) growing in preexisting cavity on the left. Right upper lobe has a large bulla (black arrow). |
view large |
 | Figure e34-49 Pulmonary arteriovenous malformation (AVM) demonstrated on reformatted CT angiogram (red arrow). |
view large |
 | Figure e34-50 Large bilateral pulmonary emboli (intravascular filling defects in contrast scan identified by red arrows). |
view large |
 | Figure e34-51 CXR of a patient with severe pulmonary hypertension. Note the enlarged pulmonary arteries (red arrows) visible on both PA and lateral films. |
view large |
 | Figure e34-52 CT scan of the same patient as in |
view large |