

PART 10: Disorders of the Cardiovascular System
SECTION 3 Disorders of Rhythm
e30 Atlas of Cardiac Arrhythmias
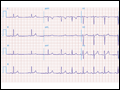 | Figure e30-1 Respiratory sinus arrhythmia, a physiologic finding in a healthy young adult. The rate of the sinus pacemaker is relatively slow at the beginning of the strip during expiration, then accelerates during inspiration and slows again with expiration. Changes are due to cardiac vagal tone modulation with breathing. |
view large |
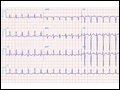
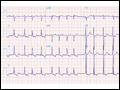
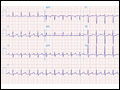 | Figure e30-2 Sinus tachycardia (110/min) with first-degree AV "block" (conduction delay) with PR interval = 0.28 s. The P wave is visible after the ST-T wave in V1−V3 and superimposed on the T wave in other leads. Atrial (non-sinus) tachycardias may produce a similar pattern, but the rate is usually faster. |
view large |
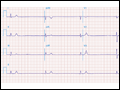
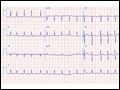
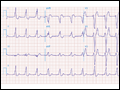
 | Figure e30-3 Sinus rhythm (P wave rate about 60/min) with 2:1 AV (second-degree) block causing marked bradycardia (ventricular rate of about 30/min). LVH is also present. |
view large |
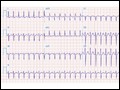
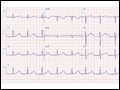
 | Figure e30-4 Sinus rhythm (P wave rate about 60/min) with 2:1 (second-degree) AV block yielding a ventricular (pulse) rate of about 30/min. Left atrial abnormality. RBBB with left anterior fascicular block. Possible inferior... |
view large |
 | Figure e30-5 Marked junctional bradycardia (25 beats/min). Rate is regular with a flat baseline between narrow QRS complexes, without evident P waves. Patient was on atenolol, with possible underlying sick sinus syndrome. |
view large |
 | Figure e30-6 Sinus rhythm at a rate of 64/min (P wave rate) with third-degree (complete) AV block yielding an effective heart (pulse) rate of 40/min. The slow, narrow QRS complexes indicate an A-V junctional escape pacemaker. Left atrial abnormality. |
view large |
 | Figure e30-7 Sinus rhythm at a rate of 90/min with advanced second-degree AV block and possible transient complete heart block with Lyme carditis. |
view large |
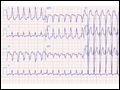
 | Figure e30-8 Multifocal atrial tachycardia with varying P-wave morphologies and P-P intervals; right atrial overload with peaked P waves in II, III, and aVF (with vertical P wave axis); superior QRS axis; slow R-wave progression with delayed transition in precordial leads in patient with severe chronic obstructive lung... |
view large |
 | Figure e30-9 NSR in a patient with Parkinson's disease. Tremor artifact, best seen in limb leads. This tremor artifact may sometimes be confused with atrial flutter/fibrillation. Borderline voltage criteria for LVH are present. |
view large |
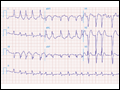
 | Figure e30-10 Atrial tachycardia with atrial rate of about 200/min (note lead V1), 2:1 AV block (conduction), and one premature ventricular complex. Also present: LVH with intraventricular conduction delay and slow precordial R-wave progression (cannot rule out prior anterior MI). |
view large |
 | Figure e30-11 Atrial tachycardia with 2:1 block. P-wave rate is about 150/min, with ventricular (QRS) rate of about 75/min. The nonconducted ("extra") P waves just after the QRS complex are best seen in lead V1. Also, note incomplete RBBB and borderline QT prolongation. |
view large |
 | Figure e30-12 Atrial tachycardia [180/min with 2:1 AV block (see lead V1)]. LVH by precordial voltage and nonspecific ST-T changes. Slow R-wave progression (V1−V4) raises consideration of prior anterior MI. |
view large |
 | Figure e30-13 AV nodal reentrant tachycardia (AVNRT) at a rate of 150/min. Note subtle "pseudo" R waves in lead aVR due to retrograde atrial activation, which occurs nearly simultaneous with ventricles in AVNRT. Left-axis deviation consistent with left anterior fascicular block (hemiblock) is also present. |
view large |
 | Figure e30-14 Atrial flutter with 2:1 AV conduction. Note atrial flutter waves, partly hidden in the early ST segment, seen, for example, in leads II and V1. |
view large |
 | Figure e30-15 Atrial flutter with atrial rate 300/min and variable (predominant 2:1 and 3:1) AV conduction. Typical flutter waves best seen in lead II. |
view large |
 | Figure e30-16 Wide complex tachycardia. Atrial flutter with 2:1 AV conduction (block) and LBBB, not to be mistaken for VT. Typical atrial flutter activity is clearly present in lead II at a cycle rate of about 320/min, with an effective ventricular rate of about 160/min. |
view large |
 | Figure e30-17 AF with LBBB. The ventricular rhythm is erratically irregular. Coarse fibrillatory waves are best seen in lead V1, with a typical LBBB pattern. |
view large |
 | Figure e30-18 AF with complete heart block and a junctional escape mechanism causing a slow regular ventricular response (45/min). The QRS complexes show an intraventricular conduction delay with left-axis deviation and LVH. Q-T (U) prolongation is also present. |
view large |
 | Figure e30-19 AF with right-axis deviation and LVH. Tracing suggests biventricular hypertrophy in a patient with mitral stenosis and aortic valve disease. |
view large |
 | Figure e30-20 WPW pre-excitation pattern, with triad of short PR, wide QRS, and delta waves. Polarity of the delta waves (slightly positive in leads V1 and V2 and most positive in lead II and lateral chest leads) is consistent with a right-sided bypass tract. |
view large |
 | Figure e30-21 AF in patient with the WPW syndrome and antegrade conduction down the bypass tract leading to a wide complex tachycardia. Rhythm is "irregularly irregular" and rate is extremely rapid (about 230/min). Not all beats are pre-excited. |
view large |
 | Figure e30-22 Accelerated idioventricular rhythm (AIVR) originating from the LV and accounting for RBBB morphology. ST elevations in the precordial leads from underlying acute MI. |
view large |
 | Figure e30-23 Prolonged (0.60 s) QT interval in a patient with hereditary long-QT syndrome. |
view large |
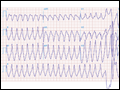 | Figure e30-24 Monomorphic VT at rate of 170/min. The RBBB morphology in V1 and the R:S ratio <1 in V6 are both suggestive of VT. The morphology of the VT is suggestive of origin from the left side of the heart, near the base (RBBB with inferior/rightward axis). Baseline artifact is present in leads... |
view large |