

PART 2: Cardinal Manifestations and Presentation of Diseases
SECTION 7 Alterations in Renal and Urinary Tract Function
e14 Atlas of Urinary Sediments and Renal Biopsies
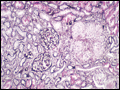
 | Figure e14-1 Minimal-change disease. In minimal-change disease, light microscopy is unremarkable (A), while electron microscopy (B) reveals podocyte injury evidenced by complete foot process effacement. (ABF/Vanderbilt Collection.) |
view large |
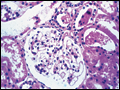
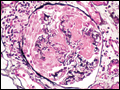
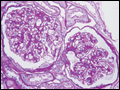
 | Figure e14-2 Focal segmental glomerulosclerosis (FSGS). There is a well-defined segmental increase in matrix and obliteration of capillary loops, the sine qua non of segmental sclerosis not otherwise specified (nos) type. (EGN/UPenn Collection.) |
view large |
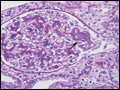
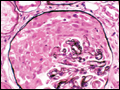
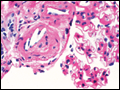
 | Figure e14-3 Collapsing glomerulopathy. There is segmental collapse of the glomerular capillary loops and overlying podocyte hyperplasia. This lesion may be idiopathic or associated with HIV infection and has a particularly poor prognosis. (ABF/Vanderbilt Collection.) |
view large |
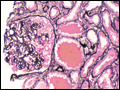
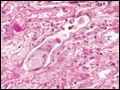
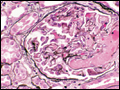
 | Figure e14-4 Hilar variant of FSGS. There is segmental sclerosis of the glomerular tuft at the vascular pole with associated hyalinosis, also present in the afferent arteriole (arrows). This lesion often occurs as a secondary response when nephron mass is lost due to, e.g., scarring from other conditions. Patients... |
view large |
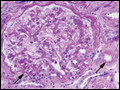
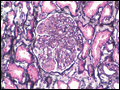
 | Figure e14-5 Tip lesion variant of FSGS. There is segmental sclerosis of the glomerular capillary loops at the proximal tubular outlet (arrow). This lesion has a better prognosis than other types of FSGS. (ABF/Vanderbilt Collection.) |
view large |
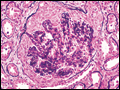 | Figure e14-6 Postinfectious (poststreptococcal) glomerulonephritis. The glomerular tuft shows proliferative changes with numerous PMNs, with a crescentic reaction in severe cases (A). These deposits localize in the mesangium and along the capillary wall in a subepithelial pattern and... |
view large |
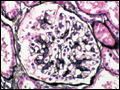
 | Figure e14-7 Membranous glomerulopathy. Membranous glomerulopathy is due to subepithelial deposits, with resulting basement membrane reaction, resulting in the appearance of spike-like projections on silver stain (A). The deposits are directly visualized by fluorescent anti-IgG,... |
view large |
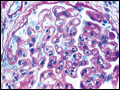
 | Figure e14-8 IgA nephropathy. There is variable mesangial expansion due to mesangial deposits, with some cases also showing endocapillary proliferation or segmental sclerosis (A). By immunofluorescence, mesangial IgA deposits are evident (B). (ABF/Vanderbilt... |
view large |
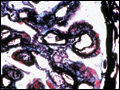
 | Figure e14-9 Membranoproliferative glomerulonephritis. There is mesangial expansion and endocapillary proliferation with cellular interposition in response to subendothelial deposits, resulting in the “tram-track” of duplication of glomerular basement membrane. (EGN/UPenn Collection.) |
view large |
 | Figure e14-10 Dense deposit disease (membranoproliferative glomerulonephritis type II). By light microscopy, there is a membranoproliferative pattern. By electron microscopy, there is a dense transformation of the glomerular basement membrane with round, globular deposits within the mesangium. By immunofluorescence, only C3 staining is... |
view large |
 | Figure e14-11 Mixed proliferative and membranous glomerulonephritis. This specimen shows pink subepithelial deposits with spike reaction, and the “tram-track” sign of reduplication of glomerular basement membrane, resulting from subendothelial deposits, as may be seen in mixed membranous and proliferative lupus nephritis (ISN/RPS... |
view large |
 | Figure e14-12 Lupus nephritis. Proliferative lupus nephritis, ISN/RPS class III (focal) or IV (diffuse), manifests as endocapillary proliferation, which may result in segmental necrosis due to deposits, particularly in the subendothelial area (A). By immunofluorescence, chunky irregular... |
view large |
 | Figure e14-13 Granulomatosis with polyangiitis (Wegener's). This pauci-immune necrotizing crescentic glomerulonephritis shows numerous breaks in the glomerular basement membrane with associated segmental fibrinoid necrosis, and a crescent formed by proliferation of the parietalepithelium. Note that the uninvolved segment of the glomerulus (at... |
view large |
 | Figure e14-14 Anti-GBM antibody-mediated glomerulonephritis. There is segmental necrosis with a break of the glomerular basement membrane and a cellular crescent (A), and immunofluorescence for IgG shows linear staining of the glomerular basement membrane with a small crescent at ~1 o'clock (B). (ABF/Vanderbilt... |
view large |
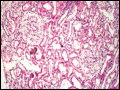
 | Figure e14-15 Amyloidosis. Amyloidosis shows amorphous, acellular expansion of the mesangium, with material often also infiltrating glomerular basement membranes, vessels, and in the interstitium, with apple-green birefringence by polarized congo red stain (A). the deposits are compose... |
view large |
 | Figure e14-16 Light chain deposition disease. There is mesangial expansion, often nodular by light microscopy (A), with immunofluorescence showing monoclonal staining, more commonly with kappa than lambda light chain, of tubules... |
view large |
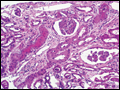
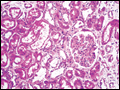
 | Figure e14-17 Light chain cast nephropathy (myeloma kidney). Monoclonal light chains precipitate in tubules and result in a syncytial giant cell reaction surrounding the casts, and a surrounding chronic interstitial nephritis with tubulointerstitial fibrosis. (ABF/Vanderbilt Collection.) |
view large |
 | Figure e14-18 Fabry's disease. Due to deficiency of α-galactosidase, there is abnormal accumulation of glycolipids, resulting in foamy podocytes by light microscopy (A). These deposits can be directly visualized by electron microscopy... |
view large |
 | Figure e14-19 Alport's syndrome and thin glomerular basement membrane lesion. In Alport's syndrome, there is irregular thinning alternating with thickened so-called basket-weaving abnormal organization of the glomerular basement membrane (A). In benign familial hematuria, or in early... |
view large |
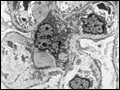
 | Figure e14-20 Diabetic nephropathy. In the earliest stage of diabetic nephropathy, only mild mesangial increase and prominent glomerular basement membranes (confirmed to be thickened by electron microscopy) are present (A). In slightly more advanced stages, more marked mesangial expansion... |
view large |
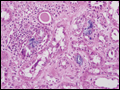
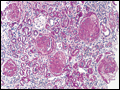 | Figure e14-21 Arterionephrosclerosis. Hypertension-associated injury often manifests extensive global sclerosis of glomeruli, with accompanying and proportional tubulointerstitial fibrosis and pericapsular fibrosis, and there may be segmental sclerosis (A). The vessels show... |
view large |
 | Figure e14-22 Cholesterol emboli. Cholesterol emboli cause cleft-like spaces where the lipid has been extracted during processing, with smooth outer contours, and surrounding fibrotic and mononuclear cell reaction in these arterioles. (ABF/Vanderbilt Collection.) |
view large |
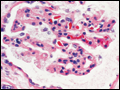
 | Figure e14-23 Hemolytic uremic syndrome. There are characteristic intraglomerular fibrin thrombi, with a chunky pink appearance (thrombotic microangiopathy). The remaining portion of the capillary tuft shows corrugation of the glomerular basement membrane due to ischemia. (ABF/Vanderbilt Collection.) |
view large |
 | Figure e14-24 Progressive systemic sclerosis. Acutely, there is fibrinoid necrosis of interlobular and larger vessels, with intervening normal vessels and ischemic change in the glomeruli (A). Chronically, this injury leads to intimal proliferation, the so-called onion-skinning appearance (B). (ABF/Vanderbilt... |
view large |
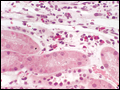
 | Figure e14-25 Acute pyelonephritis. There are characteristic intratubular plugs and casts of PMNs with inflammation extending into the surrounding interstitium, and accompanying tubular injury. (ABF/Vanderbilt Collection.) |
view large |
 | Figure e14-26 Acute tubular injury. There is extensive flattening of the tubular epithelium and loss of the brush border, with mild interstitial edema, characteristic of acute tubular injury due to ischemia. (ABF/Vanderbilt Collection.) |
view large |
 | Figure e14-27 Acute interstitial nephritis. There is extensive interstitial lymphoplasmocytic infiltrate with mild edema and associated tubular injury (A), which is frequently associated with interstitial eosinophils (B) when caused by a drug hypersensitivity reaction. (ABF/Vanderbilt... |
view large |
 | Figure e14-28 Oxalosis. Calcium oxalate crystals have caused extensive tubular injury, with flattening and regeneration of tubular epithelium (A). Crystals are well visualized as sheaves when viewed under polarized light (B). (ABF/Vanderbilt... |
view large |
 | Figure e14-29 Acute phosphate nephropathy. There is extensive acute tubular injury with intratubular nonpolarizable calcium phosphate crystals. (ABF/Vanderbilt Collection.) |
view large |
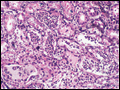
 | Figure e14-30 Sarcoidosis. There is chronic interstitial nephritis with numerous, confluent, non-necrotizing granulomas. The glomeruli are unremarkable, but there is moderate tubular atrophy and interstitial fibrosis. (ABF/Vanderbilt Collection.) |
view large |
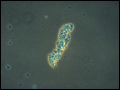
 | Figure e14-31 Hyaline cast. (ABF/Vanderbilt Collection.) |
view large |
 | Figure e14-32 Coarse granular cast. (ABF/Vanderbilt Collection.) |
view large |
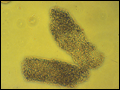 | Figure e14-33 Fine granular casts. (ABF/Vanderbilt Collection.) |
view large |
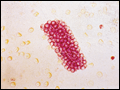 | Figure e14-34 Red blood cell cast. (ABF/Vanderbilt Collection.) |
view large |
 | Figure e14-35 WBC cast. (ABF/Vanderbilt Collection.) |
view large |
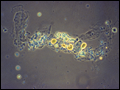
 | Figure e14-36 Triple phosphate crystals. (ABF/Vanderbilt Collection.) |
view large |
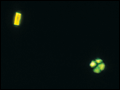 | Figure e14-37 “Maltese cross” formation in an oval fat body. (ABF/Vanderbilt Collection.) |
view large |
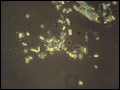
 | Figure e14-38 Uric acid crystals. (ABF/Vanderbilt Collection.) |
view large |