

PART 17: Neurologic Disorders
SECTION 3 Nerve and Muscle Disorders
388 Polymyositis, Dermatomyositis, and Inclusion Body Myositis
 | Figure 388-1 Immunopathogenesis of dermatomyositis. Activation of complement, possibly by autoantibodies (Y), against endothelial cells and formation of C3 via the classic or alternative pathway. Activated C3 leads to formation of C3b, C3bNEO, and membrane attack complexes (MAC), which are deposited in and around the endothelial cell wall of... |
view large |
 | Figure 388-2 Cell-mediated mechanisms of muscle damage in polymyositis (PM) and inclusion body myositis (IBM). Antigen-specific CD8 cells are expanded in the periphery, cross the endothelial barrier, and bind directly to muscle fibers via T cell receptor (TCR) molecules that recognize aberrantly expressed MHC-I. Engagement of co-stimulatory... |
view large |
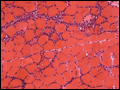 | Figure 388-3 Cross-section of a muscle biopsy from a patient with polymyositis demonstrates scattered inflammatory foci with lymphocytes invading or surrounding muscle fibers. Note lack of chronic myopathic features (increased connective tissue, atrophic or hypertrophic fibers) as seen in inclusion body myositis. |
view large |
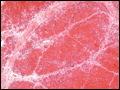 | Figure 388-4 Cross-section of a muscle biopsy from a patient with dermatomyositis demonstrates atrophy of the fibers at the periphery of the fascicle (perifascicular atrophy). |
view large |
 | Figure 388-5 Cross-sections of a muscle biopsy from a patient with inclusion body myositis demonstrate the typical features of vacuoles with lymphocytic infiltrates surrounding nonvacuolated or necrotic fibers (A), tiny endomysial deposits of amyloid visualized with crystal violet ( |
view large |