

PART 16: Endocrinology and Metabolism
SECTION 1 Endocrinology
342 Disorders of the Adrenal Cortex
 | Figure 342-1 Adrenal steroidogenesis. CYP11A1, side chain cleavage enzyme; CYP17A1, 17α-hydroxylase/17,20 lyase; POR, P450 oxidoreductase; ADX, adrenodoxin; HSD3B2, 3β-hydroxysteroid dehydrogenase type 2; CYP21A2, 21-hydroxylase; CYP11B1, 11β-hydroxylase; CYP11B2, aldosterone synthase;... |
view large |
 | Figure 342-2 Regulation of the hypothalamic-pituitary-adrenal (HPA) axis. CRH, corticotropin-releasing hormone; ACTH, adrenocorticotropic hormone. |
view large |
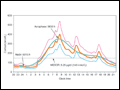 | Figure 342-3 Physiologic cortisol circadian rhythm. Circulating cortisol concentrations drop under the rhythm-adjusted mean (MESOR) in the early evening hours, with nadir levels around midnight and a rise in the early morning hours; peak levels are observed ∼8:30 a.m. (acrophase). |
view large |
 | Figure 342-4 Regulation of the renin-angiotensin-aldosterone (RAA) system. |
view large |
 | Figure 342-5 ACTH effects on adrenal steroidogenesis. ACTH, adrenocorticotropic hormone; ATP, adenosine triphosphate; CRE, cAMP response element; CREB, cAMP response element binding; MRAP, MC2R-accessory protein; StAR, steroidogenic acute regulatory [protein]. |
view large |
 | Figure 342-6 Prereceptor activation of cortisol and glucocorticoid receptor (GR) action. GRE, glucocorticoid response elements; HSP, heat shock proteins; NADPH, nicotinamide adenine dinucleotide phosphate (reduced form). |
view large |
 | Figure 342-7 Prereceptor inactivation of cortisol and mineralocorticoid receptor action. |
view large |
 | Figure 342-8 Clinical features of Cushing's syndrome. A. Note central obesity and broad, purple stretch marks (B. close-up). C. Note thin and brittle skin in an elderly patient with Cushing's. |
view large |
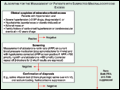
 | Figure 342-9 Management of the patient with suspected Cushing's syndrome. CHR, corticotropin-releasing hormone; DEX, dexamethasone. |
view large |
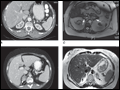 | Figure 342-10 Adrenal imaging in Cushing's syndrome. A. Adrenal CT showing normal bilateral adrenal morphology (arrows). B. MRI showing bilateral adrenal hyperplasia due to excess ACTH stimulation in Cushing's disease. |
view large |
 | Figure 342-11 Management of patients with suspected mineralocorticoid excess. Perform adrenal tumor workup (see |
view large |
 | Figure 342-12 Management of the patient with an incidentally discovered adrenal mass. F/U, follow-up. |
view large |
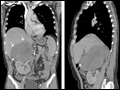 | Figure 342-13 Imaging in adrenocortical carcinoma. MRI scan with A. frontal and B. lateral views of a left adrenocortical carcinoma that was detected incidentally. CT scan with C. coronal and |
view large |
 | Figure 342-14 Clinical features of Addison's disease. Note the hyperpigmentation in areas of increased friction including (A) palmar creases, (B) dorsal foot, (C) nipples and axillary region, and ( |
view large |
 | Figure 342-15 Management of the patient with suspected adrenal insufficiency. PRA, plasma renin activity. |
view large |
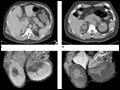 | Figure 342-16 Imaging in congenital adrenal hyperplasia (CAH). Adrenal CT scans showing homogenous bilateral hyperplasia in a young patient with classic CAH A and macronodular bilateral hyperplasia B in a middle-aged classic CAH patient with... |
view large |