

PART 16: Endocrinology and Metabolism
SECTION 1 Endocrinology
341 Disorders of the Thyroid Gland
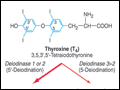 | Figure 341-1 Structures of thyroid hormones. Thyroxine (T4) contains four iodine atoms. Deiodination leads to production of the potent hormone triiodothyronine (T3), or the inactive hormone reverse T3. |
view large |
 | Figure 341-2 Regulation of thyroid hormone synthesis. Left. Thyroid hormones T4 and T3 feed back to inhibit hypothalamic production of thyrotropin-releasing hormone (TRH) and pituitary production of thyroid-stimulating hormone (TSH). TSH stimulates thyroid... |
view large |
 | Figure 341-3 Worldwide iodine nutrition. Data are from the WHO and the International Council for the Control of Iodine Deficiency Disorders (http://indorgs.virginia.edu/iccidd/mi/cidds.html). |
view large |
 | Figure 341-4 Mechanism of thyroid hormone receptor action. The thyroid hormone receptor (TR) and retinoid X receptor (RXR) form heterodimers that bind specifically to thyroid hormone response elements (TRE) in the promoter regions of target genes. In the absence of hormone, TR binds co-repressor (CoR)... |
view large |
 | Figure 341-5 Facial appearance in hypothyroidism. Note puffy eyes and thickened skin. |
view large |
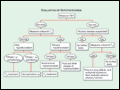 | Figure 341-6 Evaluation of hypothyroidism. TPOAb+, thyroid peroxidase antibodies present; TPOAb–, thyroid peroxidase antibodies not present; TSH, thyroid-stimulating hormone. |
view large |
 | Figure 341-7 Features of Graves' disease. A. Ophthalmopathy in Graves' disease; lid retraction, periorbital edema, conjunctival injection, and proptosis are marked. B. Thyroid dermopathy over the lateral aspects of the shins. C. Thyroid acropachy. |
view large |
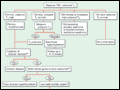 | Figure 341-8 Evaluation of thyrotoxicosis. aDiffuse goiter, positive TPO antibodies, ophthalmopathy, dermopathy; bcan be confirmed by radionuclide scan. TSH, thyroid-stimulating hormone. |
view large |
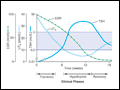 | Figure 341-9 Clinical course of subacute thyroiditis. The release of thyroid hormones is initially associated with a thyrotoxic phase and suppressed thyroid-stimulating hormone (TSH). A hypothyroid phase then ensues, with low T4 and TSH levels that are initially low but gradually incr... |
view large |
 | Figure 341-10 Activating mutations of the TSH-R. Mutations (*) that activate the thyroid-stimulating hormone receptor (TSH-R) reside mainly in transmembrane 5 and intracellular loop 3, though mutations have occurred in a variety of different locations. The effect of these mutations is to induce... |
view large |
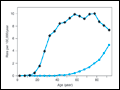 | Figure 341-11 Age-associated incidence (—♦—) and mortality (—•—) rates for invasive thyroid cancer. [Adapted from LAG Ries et al (eds): SEER Cancer Statistics Review, 1973–1996, Bethesda, National Cancer Institute, 1999.] |
view large |
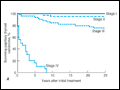 | Figure 341-12 Survival rates in patients with differentiated thyroid cancer. A. Papillary cancer, cohort of 1851 patients. I, 1107 (60%); II, 408 (22%); III, 312 (17%); IV, 24 (1%); n = 1185. B. Follicular canc... |
view large |
 | Figure 341-13 Use of recombinant human thyroid-stimulating hormone (TSH) in the follow-up of patients with thyroid cancer. Tg, thyroglobulin; rhTSH, recombinant human TSH. |
view large |
 | Figure 341-14 Approach to the patient with a thyroid nodule. See text and references for details. *About one-third of nodules are cystic or mixed solid-cystic. US, ultrasound; TSH, thyroid-stimulating hormone; FNA, fine-needle aspiration. |
view large |