

PART 14: Disorders of the Gastrointestinal System
SECTION 1 Disorders of the Alimentary Tract
293 Peptic Ulcer Disease and Related Disorders
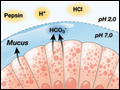
 | Figure 293-1 Diagrammatic representation of the oxyntic gastric gland. (Adapted from S Ito, RJ Winchester: Cell Biol 16:541, 1963. © The Rockefeller University Press.) |
view large |
 | Figure 293-2 Gastric parietal cell undergoing transformation after secretagogue-mediated stimulation. cAMP, cyclic adenosine monophosphate. (Adapted from SJ Hersey, G Sachs: Physiol Rev 75:155, 1995.) |
view large |
 | Figure 293-3 Components involved in providing gastroduodenal mucosal defense and repair. CCK, cholecystokinin; CRF, corticotropin-releasing factor; EGF, epidermal growth factor; HCl, hydrochloride; IGF, insulin-like growth factor; TGFα, transforming growth factor α; TRF, thyrotropin releasing factor. |
view large |
 | Figure 293-4 Schematic representation of the steps involved in synthesis of prostaglandin E2 (PGE2) and prostacyclin (PGI2). Characteristics and distribution of the cyclooxygenase (COX) enzymes 1 and 2 are also shown. TXA2, thromboxane A2. |
view large |
 | Figure 293-5 Regulation of gastric acid secretion at the cellular level. ACh, acetylcholine; ANP, atrial natriuretic peptide; CGRP, calcitonin gene-related peptide; EC, enterochromaffin; ECL, enterochromaffin-like; GRP, gastrin-releasing peptide; PACAP, pituitary adenylate-cyclase activating peptide; SST, somatostatin; VIP, vasoactive intestinal... |
view large |
 | Figure 293-6 Outline of the bacterial and host factors Important in determining H. pylori–induced gastrointestinal disease. MALT, mucosalassociated lymphoid tissue. |
view large |
 | Figure 293-7 Summary of potential mechanisms by which H.pylori may lead to gastric secretory abnormalities. D, somatostatin cell; ECL, enterochromaffin-like cell; G, G cell. (Adapted from J Calam et al: Gastroenterology 113:543, 1997.) |
view large |
 | Figure 293-8 Natural history of H. pylori-infection. (Used with permission from S Suerbaum, P Michetti: N Engl J Med 347:1175, 2002.) |
view large |
 | Figure 293-9 Mechanisms by which NSAIDs may induce mucosal injury. (Adapted from J Scheiman et al: J Clin Outcomes Management 3:23, 1996. Copyright 2003 Turner White Communications, Inc., www.turner-white.com. Used with permission.) |
view large |
 | Figure 293-10 Barium study demonstrating: A. a benign duodenal ulcer; B. a benign gastric ulcer. |
view large |
 | Figure 293-11 Endoscopy demonstrating: A. a benign duodenal ulcer; B. a benign gastric ulcer. |
view large |
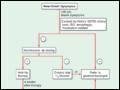 | Figure 293-12 Overview of new-onset dyspepsia. Hp, Helicobacter pylori; UBT, urea breath test; IBS, irritable bowel syndrome. (Adapted from BS Anand and DY Graham: Endoscopy 31:215, 1999.) |
view large |
 | Figure 293-13 Schematic representation of Billroth I and II procedures. |
view large |
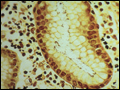 | Figure 293-14 Chronic gastritis and H. pylori organisms. Steiner silver stain of superficial gastric mucosa, showing abundant darkly stained microorganisms layered over the apical portion of the surface epithelium. Note that there is no tissue invasion. |
view large |