

PART 14: Disorders of the Gastrointestinal System
SECTION 1 Disorders of the Alimentary Tract
291 Gastrointestinal Endoscopy
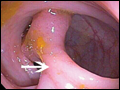
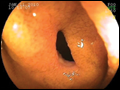
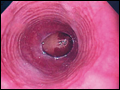
 | Figure 291-1 Duodenal ulcers. Ulcer with a clean base. Ulcer with a visible vessel (arrow) in a patient with recent hemorrhage. |
view large |
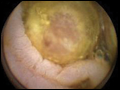
 | Figure 291-2 Gastric ulcers. A. Benign gastric ulcer. B. Malignant gastric ulcer involving greater curvature of stomach. |
view large |
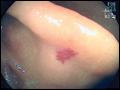
 | Figure 291-3 Barrett's esophagus. A. Pink tongues of Barrett's mucosa extending proximally from the gastroesophageal junction. B. Barrett's esophagus with a suspicious nodule (arrow) identified during endoscopic surveillance. C.... |
view large |
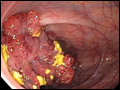
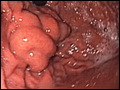
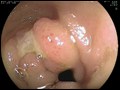
 | Figure 291-4 Causes of colitis. A. Chronic ulcerative colitis with diffuse ulcerations and exudates. B. Severe Crohn's colitis with deep ulcers. C. Pseudomembranous colitis with yellow, adherent pseudomembranes. D. Ischemic colitis with patchy mucosal edema, subepithelial hemorrhage, and... |
view large |
 | Figure 291-5 Colonic polyps. A. Pedunculated colon polyp on a thick stalk covered with normal mucosa (arrow). B. Sessile rectal polyp. |
view large |
 | Figure 291-6 Colon adenocarcinoma growing into the lumen. |
view large |
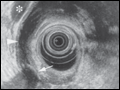
 | Figure 291-7 Capsule endoscopy image of jejunal vascular ectasia. |
view large |
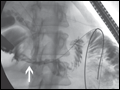
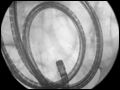 | Figure 291-8 Radiograph of a double-balloon enteroscope in the small intestine. |
view large |
 | Figure 291-9 Nonsteroidal anti-inflammatory (NSAID)-induced proximal ileal stricture diagnosed by double-balloon endoscopy. A. Ileal stricture causing obstructive symptoms. B. Balloon dilatation of the ileal stricture. C. Appearance of stricture after... |
view large |
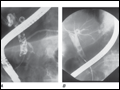 | Figure 291-10 Endoscopic retrograde cholangiopancreatography (ERCP) for bile duct stones with cholangitis. A. Faceted bile duct stones are demonstrated in the common bile duct. B. After endoscopic sphincterotomy, the stones are extracted with a Dormia basket. A small abscess communicates with the left hepatic... |
view large |
 | Figure 291-11 Endoscopic sphincterotomy. A. A normal-appearing ampulla of Vater. B. Sphincterotomy is performed with electrocautery. C. Bile duct stones are extracted with a balloon catheter. D. Final appearance of the... |
view large |
 | Figure 291-12 Endoscopic diagnosis, staging, and palliation of hilar cholangiocarcinoma. A. Endoscopic retrograde cholangiopancreatography (ERCP) in a patient with obstructive jaundice demonstrates a malignant-appearing stricture of the biliary confluence extending into the left and right intrahepatic ducts. |
view large |
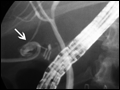 | Figure 291-13 Bile leak (arrow) from a duct of Luschka after laparoscopic cholecystectomy. Contrast leaks from a small right intrahepatic duct into the gallbladder fossa, then flows into the pigtail of a percutaneous drainage catheter. |
view large |
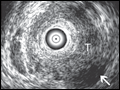
 | Figure 291-14 Local staging of gastrointestinal cancers with endoscopic ultrasound. In each example the white arrowhead marks the primary tumor and the black arrow indicates the muscularis propria (mp) of the intestinal wall. A. T1 gastric cancer. The tumor does not invade the mp. B. |
view large |
 | Figure 291-15 Endoscopic ultrasound (EUS)-guided fine-needle aspiration (FNA). A. Ultrasound image of a 22-gauge needle passed through the duodenal wall and positioned in a hypoechoic pancreatic head mass. B. Micrograph of aspirated malignant cells. (Image B courtesy of Dr. Michael R. Henry; with... |
view large |
 | Figure 291-16 Stigmata of hemorrhage in peptic ulcers. A. Gastric antral ulcer with a clean base. B. Duodenal ulcer with flat pigmented spots. C. Duodenal ulcer with a dense adherent clot. D. Gastric ulcer with a pigmented protuberance/visible vessel. E. Duodenal ulcer with active spurting ( |
view large |
 | Figure 291-17 Esophageal varices. |
view large |
 | Figure 291-18 Gastric fundic varices. |
view large |
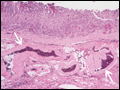 | Figure 291-19 Dieulafoy's lesion. A. Actively spurting jejunal Dieulafoy's lesion. There is no underlying mucosal lesion. B. Histology of a gastric Dieulafoy's lesion. A persistent caliber artery (arrows) is present in the gastric submucosa, immediately beneath the... |
view large |
 | Figure 291-20 Mallory-Weiss tear at the gastroesophageal junction. |
view large |
 | Figure 291-21 Gastrointestinal vascular ectasias. A. Gastric antral vascular ectasia (“watermelon stomach”) characterized by stripes of prominent flat or raised vascular ectasias. B. Cecal vascular ectasias. C. Radiation-induced vascular ectasias of the rectum in a patient previously treated for prostate... |
view large |
 | Figure 291-22 Colonic diverticula. |
view large |
 | Figure 291-23 Esophageal food (meat) impaction. |
view large |
 | Figure 291-24 Biliary and duodenal self-expanding metal stents (SEMS) for obstruction caused by pancreatic cancer. A. Endoscopic retrograde cholangiopancreatography (ERCP) demonstrates a distal bile duct stricture (arrow). B. A biliary SEMS is placed. C. Contrast injection demonstrates a duodenal stricture (arrow). D. Biliary and duodenal SEMS... |
view large |
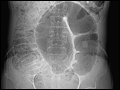 | Figure 291-25 Sigmoid volvulus with the characteristic radiologic appearance of a “bent inner tube.” |
view large |
 | Figure 291-26 Acute colonic pseudoobstruction. A. Acute colonic dilatation occurring in a patient soon after knee surgery. B. Colonoscopic placement of decompression tube with marked improvement in colonic dilatation. |
view large |
 | Figure 291-27 Obstructing colonic carcinoma. A. Colonic adenocarcinoma causing marked luminal narrowing of the descending colon. B. Endoscopic placement of a self-expanding metal stent. C. Radiograph of expanded stent across the obstructing tumor with a residual waist (arrow). (Image A courtesy of Dr. Glenn Alexander; with... |
view large |
 | Figure 291-28 Methods of bile duct imaging. Arrows mark bile duct stones. Arrowheads indicate the common bile duct, and the asterisk marks the portal vein. A. Endoscopic ultrasound (EUS). B. Magnetic resonance cholangiopancreatography (MRCP). C. Helical computed... |
view large |
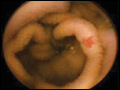
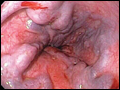
 | Figure 291-29 Causes of esophagitis. A. Severe reflux esophagitis with mucosal ulceration and friability. B. Cytomegalovirus esophagitis. C. Herpes simplex virus esophagitis with target-type shallow ulcerations. D. Candida esophagitis with white plaques adherent to the esophageal... |
view large |
 | Figure 291-30 Peptic esophageal stricture associated with ulceration and scarring of the distal esophagus. |
view large |
 | Figure 291-31 Schatzki's ring at the gastroesophageal junction. |
view large |
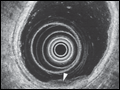
 | Figure 291-32 Eosinophilic esophagitis with multiple circular rings of the esophagus creating a corrugated appearance, and an impacted grape at the narrowed esophagogastric junction. The diagnosis requires biopsy with histologic finding of >15–20 eosinophils/high power field. |
view large |
 | Figure 291-33 Scalloped duodenal folds in a patient with celiac sprue. |
view large |
 | Figure 291-34 Capsule endoscopy images of a mildly scalloped jejunal fold (left) and an ileal tumor (right) in a patient with celiac sprue. (Images courtesy of Dr. Elizabeth Rajan; with permission.) |
view large |
 | Figure 291-35 A. Mid-jejunal vascular ectasia identified by double-balloon endoscopy. B. Ablation of vascular ectasia with argon plasma coagulation. |
view large |
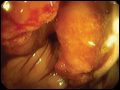
 | Figure 291-36 Innumerable colon polyps of various sizes in a patient with familial adenomatous polyposis syndrome. |
view large |
 | Figure 291-37 Virtual colonoscopy image of a colon polyp (arrow). (Image courtesy of Dr. Jeff Fidler; with permission.) |
view large |
 | Figure 291-38 Ulcerated ileal carcinoid tumor. |
view large |
 | Figure 291-39 Internal hemorrhoids with bleeding (arrow) as seen on a retroflexed view of the rectum. |
view large |
 | Figure 291-40 Management of antithrombotic agents for elective endoscopic procedures. Higher-risk procedures for bleeding: Ploypectomy, biliary or pancreatic sphincterotomy, therapeutic balloon-assisted enteroscopy, PEG placement, pneumatic or bougie dilatation, treatment of varices, endoscopic hemostasis, tumor ablation by any technique, ... |
view large |
 | Figure 291-41 Management of antithrombotic agents for urgent endoscopic procedures. Higher-risk procedures for bleeding: Polypectomy, biliary or pancreatic sphincterotomy, therapeutic balloon-assisted entero-scopy, PEG placement, pneumatic or bougie dilatation, treatment of varices, endoscopic hemostasis, tumor ablation by any technique,... |
view large |