

PART 10: Disorders of the Cardiovascular System
SECTION 4 Disorders of the Heart
237 Valvular Heart Disease
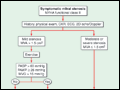 | Figure 237-1 Management strategy for patients with mitral stenosis (MS) and mild symptoms. †There is controversy as to whether patients with severe MS (MVA <1 cm2) and severe pulmonary hypertension (PH) (PASP >60 mmHg) should undergo percutaneous mitral balloon valvotomy... |
view large |
 | Figure 237-2 Inoue balloon technique for percutaneous mitral balloon valvotomy. A. After transseptal puncture, the deflated balloon catheter is advanced across the interatrial septum, then across the mitral valve and into the left ventricle. |
view large |
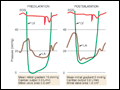 | Figure 237-3 Simultaneous left atrial (LA) and left ventricular (LV) pressure before and after percutaneous mitral balloon valvuloplasty (PMBV) in a patient with severe mitral stenosis. (Courtesy of Raymond G. McKay, MD; with permission.) |
view large |
 | Figure 237-4 Management strategy for patients with chronic severe nonischemic mitral regurgitation. *Mitral valve (MV) repair may be performed in asymptomatic patients with normal left ventricular (LV) function if performed by an experienced surgical team and if the likelihood of successful MV repair... |
view large |
 | Figure 237-5 Clip used to grasp the free edges of the anterior and posterior leaflets in their mid-sections during percutaneous repair of selected patients with mitral regurgitation. (Courtesy of Abbott Vascular. © 2010 Abbott Laboratories. All rights reserved.) |
view large |
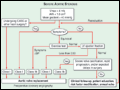
 | Figure 237-6 Pathogenesis of calcific aortic stenosis. Inflammatory cells infiltrate across the endothelial barrier and release cytokines that act on fibroblasts to promote cellular proliferation and matrix remodeling. LDL is oxidatively modified and taken up by macrophage scavengers to become foam... |
view large |
 | Figure 237-7 Management strategy for patients with severe aortic stenosis. Preoperative coronary angiography should be performed routinely as determined by age, symptoms, and coronary risk factors. Cardiac catheterization and angiography may also be helpful when there is a discrepancy between clinical... |
view large |
 | Figure 237-8 A. Balloon-expandable and B and self-expanding valves for percutaneous aortic valve replacement. B, inflated balloon; N, nose cone; V, valve. (Part A, courtesy of Edwards Lifesciences, Irvine, CA; with permission. RetroFlex 3 is a... |
view large |
 | Figure 237-9 Twelve-month outcomes following percutaneous aortic valve replacement. (Adapted from JG Webb et al: Circulation 116:755, 2007; with permission.) |
view large |
 | Figure 237-10 Management strategy for patients with chronic severe aortic regurgitation. Preoperative coronary angiography should be performed routinely, as determined by age, symptoms, and coronary risk factors. Cardiac catheterization and angiography may also be helpful when there is a discrepancy... |
view large |
 | Figure 237-11 Valve-sparing aortic root reconstruction (David procedure). (From P Steltzer et al (eds): Valvular Heart Disease: A Companion to Braunwald's Heart Disease, 3rd ed, |
view large |